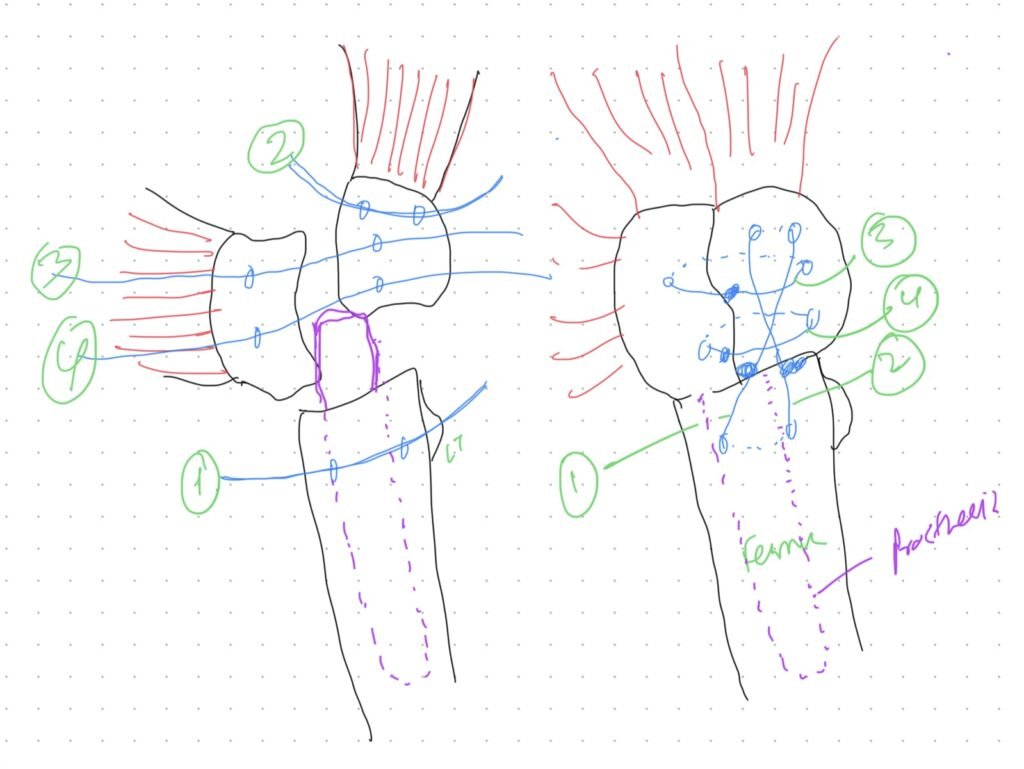
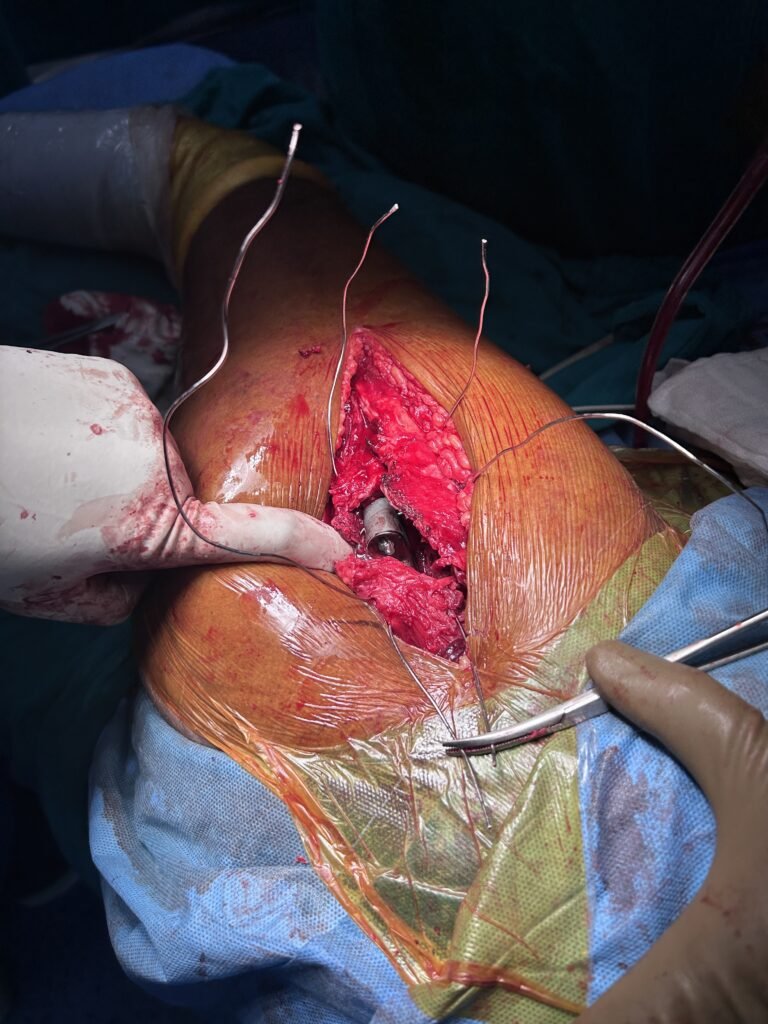
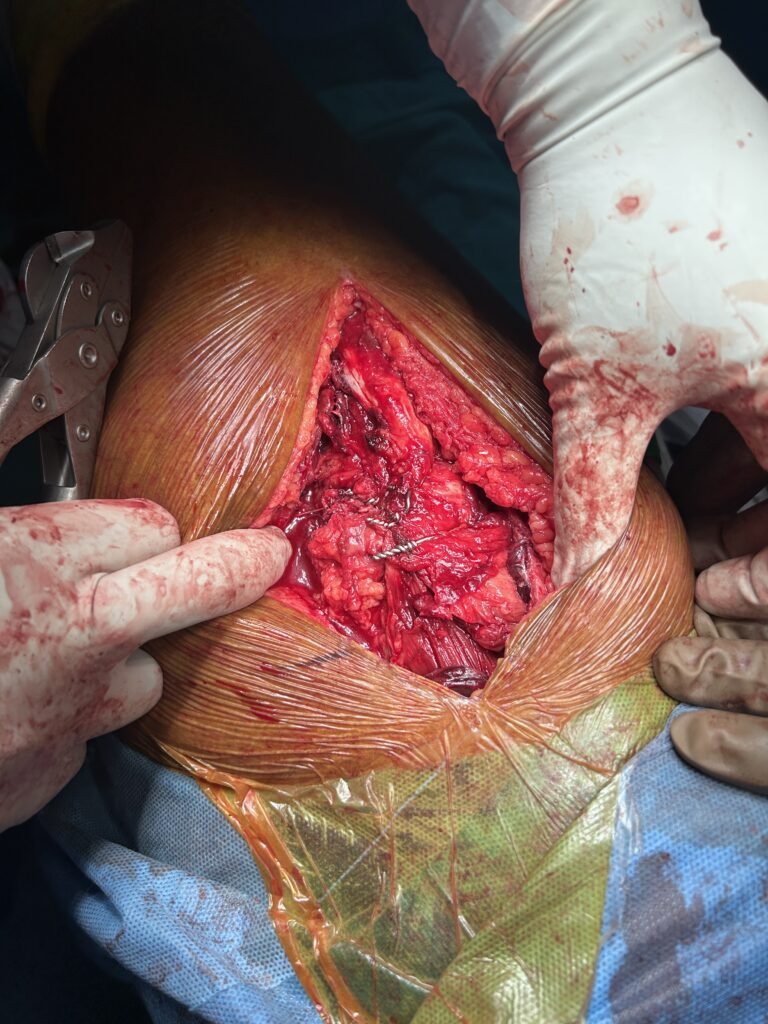
In Past few months i have got many elderly patients with comminuted intertrochanteric fracutre. While suffering few failures after doing PFN due to diffucult reduction, osteoporosis, i have switched to doing primary hip replacement is such patient speciallly in those with comorbidity and obesity. I face difficulty approaching the hip every time because of different fracture patterns and soft tissue detachment configuration. Commonly i encountered this type of fracture where one part GT is detached from vastus and migrated up , second part attached to vastus and a 3 LT fragment. I have gotten good result with this configuration of GT wiring where i am unable to reduce the GT fragment properly.
TBW brings the abductor fragment down and normal wiring approximates the remaining ends. Over all gives a good stability.